After 11 years of hosting the International Research Community on Multimorbidity, the Université de Sherbrooke has passed on the baton to the University of Glasgow. Led by Martin Fortin and colleagues, the website was started as a place to report on multimorbidity research taking place internationally. Since the inception in 2011, with only a small group of members, the international community and the amount of outstanding research in this field has grown dramatically. We want to continue to recognise this by sharing your news and events on multimorbidity research. The blog posts and updates of the library of multimorbidity literature will continue. We will have an archive of past blog posts coming soon and, in the meantime, the Université de Sherbrooke website will remain visible, please see the link on our new website. Please let us know via our email address (multimorbidityblog@glasgow.ac.uk) when you have news to share with this community or if you have ideas for the type of material you would like us to share.
We are very grateful to Martin Fortin and José Almirall-Collazo for sharing their knowledge and tips on the community onto us. Bhautesh Jani and Barbara Nicholl will lead the website at Glasgow and will strive to make it a shared space for the international community to share research activity on multimorbidity. We look forward to seeing some of you at the North American Primary Care Research Group annual meeting in November. Please sign up to joint our mailing list here https://forms.office.com/r/QtNG3Vthvs
Dear all, We are organizing an International Symposium on Multimorbidity in Amsterdam, the Netherlands. The meeting will be held in hybrid form. Speakers include: Prof Dr Chris Salisbury, Dr Amaia Calderón-Larrañaga, Dr Rene Melis and many others! Please find the full program, and options for registration here:
By Jonathan Stokes, Peter Bower, Bruce Guthrie, Susan Smith, Tom Blakeman, Chris Salisbury
Dear International Research Community on Multimorbidity,
We are currently conducting a project titled, “Developing an updated agenda for Primary Care research on Multiple Long-Term Conditions (Multimorbidity)”.
As part of this, we are developing a Delphi-like online prioritisation survey. If you would be interested in giving your view on what primary care research areas should be prioritised and:
You’re an academic primary care professional (we’re interested in views of both clinical and non-clinical researchers)
You conduct multimorbidity research in high-income country setting(s) (as we expect the challenges are quite different in LMICs)
Please contact Jonathan Stokes (Jonathan.m.stokes@manchester.ac.uk) to register your interest. Round one of the survey is likely to take place in early September, with round two to follow thereafter.
Thank you in advance for your interest and participation.
By Iris Ho and Bruce Guthrie on behalf of all authors
Measuring multimorbidity is complex. We have recently published papers from a Health Data Research UK funded study which report a systematic review of how multimorbidity is measured in the literature, and an international Delphi study seeking to identify consensus on how multimorbidity should be measured.
The systematic review examined how 566 studies defined and measured multimorbidity, finding very large variation. One in eight studies did not report which conditions were included in their multimorbidity measure. Where reported, then the number of conditions included varied from two to 285 (median 17, IQR 11-23). Most studies included at least one cardiovascular condition (98%), metabolic condition (97%), respiratory condition (93%), or musculoskeletal condition (88%). Only 78% included any mental health condition, and many other body systems were infrequently included (eg haematological conditions 24%). Only eight individual conditions (all of them physical conditions) were included by more than half of studies (diabetes, stroke, cancer, chronic obstructive pulmonary disease, hypertension, coronary heart disease, chronic kidney disease, and heart failure). (Ho et al https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667(21)00107-9/fulltext).
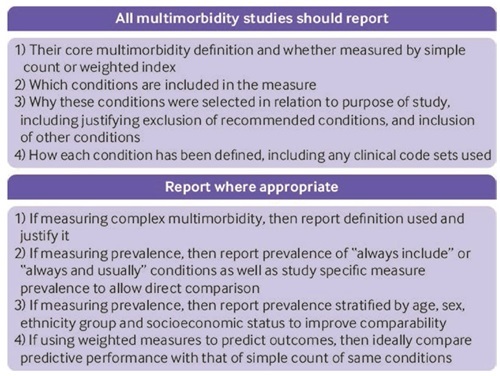
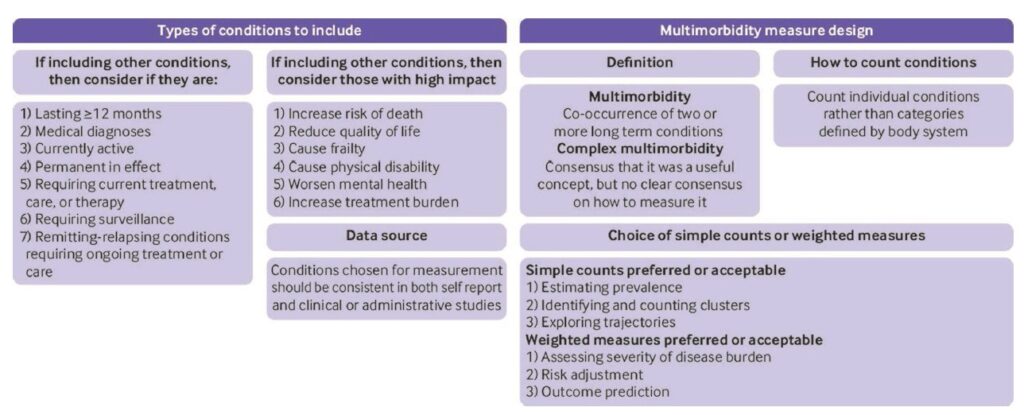
We concluded that there was an urgent need for more consistency in the field, and therefore carried out a three round Delphi consensus study with 150 professionals and 25 public panel members in round 1. Highlights of the results were that there was consensus that multimorbidity should be defined as two or more conditions. Although ‘complex multimorbidity’ (eg 3+ conditions, or 3+ conditions from 3+ body systems) was perceived as potentially useful, there was no consensus on how to define it, highlighting the need for more research into alternative definitions. Simple counts of conditions were preferred for estimating prevalence and examining clusters or trajectories, and weighted measures were preferred for risk adjustment and outcome prediction. Reflecting the variability in the systematic review, there was consensus that studies needed to be more consistent in their reporting (figure and table below are reproduced from the paper under the CC-BY licence).
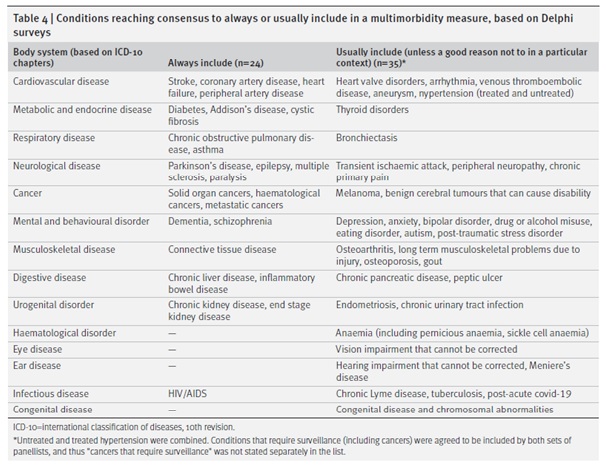
Finally, there was consensus for 24 conditions that should “always” be included in multimorbidity measurement and 35 that should be “usually included (unless a good reason not to in a particular context)”. We recognise that choices should reflect context and local condition prevalence so the combined ‘always or usually include’ list can be seen as a core set of conditions with scope for local adaptation (Ho et al https://bmjmedicine.bmj.com/content/1/1/e000247).
Further research and consensus is needed to define codelists or other diagnostic criteria for the listed conditions, to examine the relative value of unweighted vs weighted measures, and to understand the additional value (if any) of different definitions of complex multimorbidity.
Like all consensus recommendations, we expect that many researchers will find at least a few items that they disagree with. BG for example finds the non-inclusion of depression in the ‘always include’ list perplexing (albeit it only just failed to reach the pre-specified 70% consensus level for inclusion, but easily reached consensus for ‘usually include’). However, unless there are pressing and explicitly justified reasons to vary from the consensus, we think it would ideal for researchers in this field to align where feasible. We hope that these studies will be interesting and useful to the research community, and welcome any feedback.
By Søren T. Skou, Frances S. Mair, Martin Fortin,Bruce Guthrie, Bruno P. Nunes, J. Jaime Miranda, Cynthia M. Boyd, Sanghamitra Pati, Sally Mtenga, Susan M. Smith
An international, interdisciplinary group of researchers and clinicians from nine different countries across five continents recently completed a review on multimorbidity, which was published in Nature Reviews Disease Primers, a top five general medical journal (journal impact factor of 65) [1]. The review, called a Primer, provides a global overview of a specific medical field as well as outlining future directions and research questions. Primers provide clinicians and researchers around the world with an understanding of the epidemiology, mechanisms/pathophysiology, prevention, diagnosis, and treatment for a specific medical condition or concept. The process leading to the publication of the multimorbidity Primer started in January 2021 when the authors drafted a pre-submission inquiry, which was sent to the journal. After this the journal invited us to prepare a manuscript for submission, which was sent for peer review and finally accepted after several rounds of revision and published in July 2022. We put a lot of work into writing the manuscript, but it was a very rewarding process as it gave us an opportunity to collaborate and review the latest literature on multimorbidity and develop ideas for future projects together. The primer underlined the burden of multimorbidity on individuals, carers and society, especially in socioeconomically deprived communities. Furthermore, it highlighted the complex, interrelated and multilevel mechanisms involved in the development of multimorbidity, including aging, biological mechanisms, and broader socio-determinants of health. Evidence for prevention and treatment is still limited. While there is more literature on interventions there is still no clear evidence to guide clinical practice and policy. The Primer suggests that interventions for multimorbidity may be person-centred, complex and multifaceted, and among other things focus on psychosocial and behavioural factors. The Primer also highlighted the need for further research particularly in low- and middle-income countries. Finally, the Primer calls for a change in focus for clinical practice and training to become more multimorbidity focused along with a shift in healthcare to support proper prevention and management of multimorbidity. To read more, you can find the full Primer for free here: https://rdcu.be/cRBzm You will also be able to find an infographic associated with the Primer here: https://rdcu.be/cTqpw It provides a quick overview of the review findings for your clinical practice or workspace.
1 Multimorbidity. Skou ST, Mair FS, Fortin M, Guthrie B, Nunes BP, Miranda JJ, Boyd CM, Pati S, Mtenga S, Smith SM. Nat Rev Dis Primers. 2022 Jul 14;8(1):48. doi: 10.1038/s41572-022-00376-4.
Our search for papers on multimorbidity that were published during the period January-April 2022 has been completed. As in previous searches, we have prepared a PDF file that can be accessed following this link. Probably, there are some publications that were not detected by our search strategy using the terms “multimorbidity”, “multi-morbidity” and the expressions “multiple chronic diseases” and “multiple long-term conditions” in PubMed (https://www.ncbi.nlm.nih.gov/pubmed), but we are sure that most publications on the subject are included in the list. All references are also included in our library. Feel free to share with anyone interested in multimorbidity.
Our search for papers on multimorbidity that were published during the period September-December 2021 has been completed. As in previous searches, we have prepared a PDF file that can be accessed following this link.
Probably, there are some publications that were not detected by our search strategy using the terms “multimorbidity”, “multi-morbidity” and the expressions “multiple chronic diseases” and “multiple long-term conditions” in PubMed (https://www.ncbi.nlm.nih.gov/pubmed), but we are sure that most publications on the subject are included in the list. All references are also included in our library. Feel free to share with anyone interested in multimorbidity.
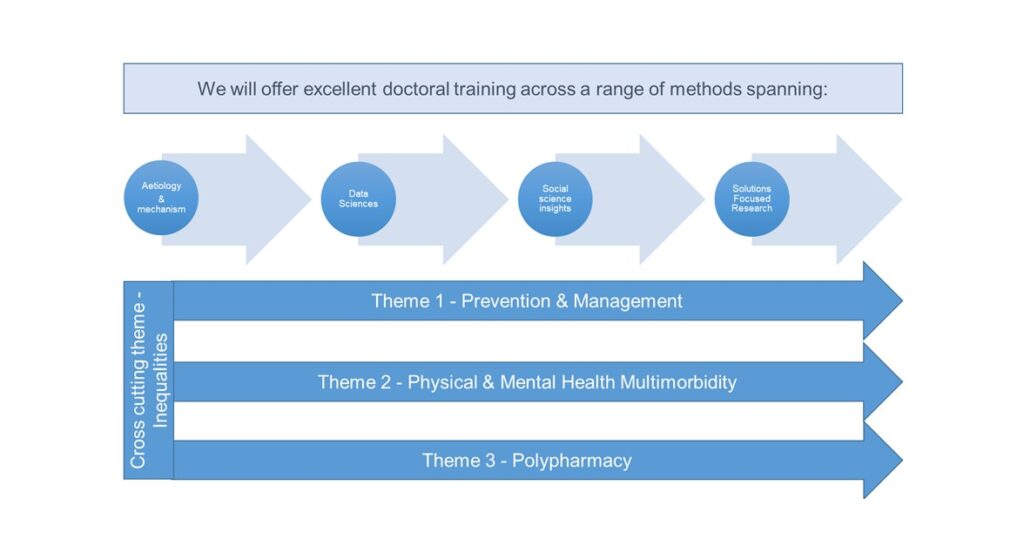
A new Multimorbidity PhD programme for health professionals, funded by Wellcome Trust, has recently been launched in Scotland. The new PhD programme is led by the University of Glasgow in collaboration with the Universities of Dundee, Edinburgh and St Andrews, and aims to train a new generation of healthcare professionals with transferable skills for academic, clinical and policy roles, with a focus on generation of evidence that will enhance understanding of the determinants of multimorbidity and inform development of patient-focused interventions to improve care and outcomes. The PhD Fellows will be recruited from a range of clinical and health professional backgrounds and be offered exceptional opportunities for clinical research across a range of specialisms, from data science and epidemiology, to applied clinical research in a unique collaborative training environment. Our vision is to create a cohort of academic health professionals, including doctors, nurses, pharmacists, dentists, clinical psychologists and allied health professionals, for whom interdisciplinary and integrated thinking is the norm, with the skills to bridge research gaps and overcome the challenges posed by multimorbidity. Hosted in the Scottish societal context, where multimorbidity is a key health concern, but examining globally relevant problems, it will promote development of a critical mass of multimorbidity researchers empowered to find ways to prevent multimorbidity, discover pathways tractable to novel intervention and optimise management. The programme builds on the strengths of the partner institutions, to create a rich, multidisciplinary environment that will equip a new generation of researchers with a broad range of methodological skills that will enable them to promote new thinking on this complex topic. The programme has three research themes: Prevention and Management; Physical and Mental Health Multimorbidity and Polypharmacy with Inequalities as a cross-cutting theme.
Fellows will participate in a range of cohort-building activities aimed at developing a community and broadening understanding of research and interdisciplinary collaboration. Patient and Public Involvement (PPI) and Knowledge Exchange (KE) skill development are core elements of the planned development programme for Fellows. The Programme will be recruiting for new Fellows annually for the next 5 years, during this time we expect to support 34 Fellows, making this the largest Multimorbidity PhD Programme for Health Professionals globally. We have just recruited our first cohort of Fellows who will commence in November 2022. Further details of the programme and the types of research projects being offered can be found here: https://www.gla.ac.uk/colleges/mvls/graduateschool/multimorbidity/.
By Martin Fortin, Moira Stewart, José Almirall, and Priscilla Beaupré
Patients with multimorbidity need a new kind of health care. Numerous rigorous studies using randomized controlled designs (RCTs) have been conducted to demonstrate effectiveness of interventions aimed at improving outcomes for patient with multimorbidity in primary care, but most of them have reported neutral effects or mixed results. Nevertheless, these studies offer a valuable source of information to learn from in order to pave the way for future research in this area in primary care. We conducted a scoping review [1] to include current up-to-date state-of-the-art studies in primary care published from 2019 until 2021 in order to synthesize and analyze the most recent RCTs and to identify the factors that may have contributed to the success or lack of success. Special attention was given to four elements of the intervention: 1) its description and content; 2) the context in which it was deployed; 3) the evaluation design chosen to test the effectiveness, and 4) the intervention’s implementation. Nine articles reporting on six RCTs studies were included in the review. The findings were mixed, with primary outcomes showing no differences between intervention and control groups in four of the six but differences in secondary outcomes in all six. All studies involved family practice patients but interventions took place at different sites, and the time between the beginning of the intervention and the time of evaluation of outcomes varied across studies. Authors reported issues regarding the need for training of care teams, the roles and composition of the teams, the selection of patients and implementation barriers of the complex interventions in trying contexts with not enough time for the changes required. This scoping review identified several lessons on planning for future intervention studies on multimorbidity in primary care. Interdisciplinary teams as the basis for most interventions, while recommended, may need more support by policy and practice leadership to be successfully deployed and evaluated. The randomized controlled design may not be the best evaluation design given the complexity of the interventions; alternative designs should be considered in which qualitative components are included. Special attention should be given to outcome measures ensuring that they are better aligned to patient goals. Selection of patients was prone to bias toward the less needy and this may hamper the ability to document effectiveness and raises questions about equity in research. Implementation of the interventions needs special attention and enough time to gel.
1-Fortin M, Stewart M, Almirall J and Beaupré P (2022) Challenges in Multimorbidity Research: Lessons Learned From the Most Recent Randomized Controlled Trials in Primary Care. Front. Med. 9:815783. doi: 10.3389/fmed.2022.815783
Different attempts have been made to create effective interventions in primary care for people with multimorbidity, being the predominant intervention element a change to the organization of care delivery. However, these interventions have obtained mixed results. We recently reported the results of a trial assessing the effectiveness of a multifaceted intervention based on a change in care delivery for patients with three or more chronic conditions [1]. After four months, the intervention showed a neutral effect on the primary outcomes and substantial improvement in two health behaviors as secondary outcomes. However, the effect of the intervention after a longer period of time was not known. We have now reported the one-year outcomes after exposure to the intervention, combining all participants in one single group that received the intervention, to document its long-term association with measures of self-care, quality of life and health-related behaviors [2]. Changes in these measures were also analyzed across age-, number of chronic conditions-, income-, and gender-based subgroups to explore factors potentially associated with variation in response to the intervention and help guide the development of more targeted interventions in the future.
We observed that one year after the
intervention, the domain of emotional wellbeing of the Health Education
Questionnaire (heiQ), improved significantly. However, we also observed
deterioration in the domain of health services navigation of the heiQ. Improvement
was also observed for the measures of the VR-12 (Veteran RAND-12 Health Survey)
physical component, VR-12 mental component, in moderate to severe psychological
distress measured with the Kessler six item Psychological Stress Scale (K6), and
healthy eating.
Subgroup analyses in this exploratory study
suggest that younger patients, those with lower number of chronic conditions or
higher incomes may respond better in relation to self-management, health status
and health behaviors. This suggests that future interventions should be
tailored to patients’ characteristics including age, sex, income and number of
conditions.
1. Fortin M, Stewart
M, Ngangue P, Almirall J, Belanger M, Brown JB, et al. Scaling Up
Patient-Centered Interdisciplinary Care for Multimorbidity: A Pragmatic
Mixed-Methods Randomized Controlled Trial. Ann
Fam Med (2021) 19(2):126-34. doi: 10.1370/afm.2650.
2. Fortin
M, Stewart M, Almirall J, Berbiche D, Belanger M, Katz A, et al. One year
follow-up and exploratory analysis of a patient-centered interdisciplinary care
intervention for multimorbidity. J Comorb
(2021) 11:26335565211039780. doi: 10.1177/26335565211039780.